(Note: My apologies for the sarcastic tone of this post. I am not really congratulating anybody here!)
Dr. Nick Delgado shows us in this YouTube video how to "become diabetic" in 6 hours!
I must admit that I liked the real-time microscope imaging, and wish he had shown us more of that.
But really!
After consulting with my mentor, the MIMIW, I was reminded that there is at least one post on this blog that shows how one can "become diabetic" in just over 60 minutes – that is, about 6 times faster than using the technique described by Dr. Delgado.
The technique used in the post mentioned above is called "intense exercise", which is even believed to be health-promoting! (Unlike drinking olive oil as if it was water, or eating white bread.)
The advantage of this technique is that one can "become diabetic" by doing something healthy!
Thanks Dr. Delgado, your video ranks high up there, together with this Ali G. video, as a fine example of how to bring real science to the masses.
Tuesday, August 31, 2010
Sunday, August 29, 2010
Heavy physical activity may significantly reduce heart disease deaths, especially after age 45
The idea that heavy physical activity is a main trigger of heart attacks is widespread. Often endurance running and cardio-type activities are singled out. Some people refer to this as “death by running”. Others think that strength training has a higher lethal potential. We know based on the Oregon Sudden Unexpected Death Study that this is a myth.
Here is some evidence that heavy physical activity in fact has a significant protective effect. The graph below, from Brooks et al. (2005) shows the number of deaths from coronary heart disease, organized by age group, in longshoremen (dock workers). The shaded bars represent those whose level of activity at work was considered heavy. The unshaded bars represent those whose level of activity at work was considered moderate or light (essentially below the “heavy” level).
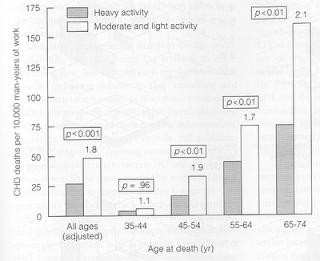
The data is based on an old and classic study of 6351 men, aged 35 to 74 years, who were followed either for 22 years, or to death, or to the age of 75. It shows a significant protective effect of heavy activity, especially after age 45. The numbers atop the unshaded bars reflect the relative risk of death from coronary heart disease in each age group. For example, in the age group 65-74, the risk among those not in the heavy activity group is 110 percent higher (2.1 times higher) than in the heavy activity group.
It should be noted that this is a cumulative effect, of years of heavy activity. Based on the description of the types of activities performed, and the calories spent, I estimate that the heavy activity group performed the equivalent of a few hours of strength training per week, plus a lot of walking and other light physical activities. The authors of the study concluded that “… repeated bursts of high energy output established a plateau of protection against coronary mortality.”
Heavy physical activity may not make you lose much weight, but has the potential to make you live longer.
Reference:
Brooks, G.A., Fahey, T.D., & Baldwin, K.M. (2005). Exercise physiology: Human bioenergetics and its applications. Boston, MA: McGraw-Hill.
Here is some evidence that heavy physical activity in fact has a significant protective effect. The graph below, from Brooks et al. (2005) shows the number of deaths from coronary heart disease, organized by age group, in longshoremen (dock workers). The shaded bars represent those whose level of activity at work was considered heavy. The unshaded bars represent those whose level of activity at work was considered moderate or light (essentially below the “heavy” level).

The data is based on an old and classic study of 6351 men, aged 35 to 74 years, who were followed either for 22 years, or to death, or to the age of 75. It shows a significant protective effect of heavy activity, especially after age 45. The numbers atop the unshaded bars reflect the relative risk of death from coronary heart disease in each age group. For example, in the age group 65-74, the risk among those not in the heavy activity group is 110 percent higher (2.1 times higher) than in the heavy activity group.
It should be noted that this is a cumulative effect, of years of heavy activity. Based on the description of the types of activities performed, and the calories spent, I estimate that the heavy activity group performed the equivalent of a few hours of strength training per week, plus a lot of walking and other light physical activities. The authors of the study concluded that “… repeated bursts of high energy output established a plateau of protection against coronary mortality.”
Heavy physical activity may not make you lose much weight, but has the potential to make you live longer.
Reference:
Brooks, G.A., Fahey, T.D., & Baldwin, K.M. (2005). Exercise physiology: Human bioenergetics and its applications. Boston, MA: McGraw-Hill.
Tuesday, August 24, 2010
Lipotoxicity or tired pancreas? Abnormal fat metabolism as a possible precondition for type 2 diabetes
The term “diabetes” is used to describe a wide range of diseases of glucose metabolism; diseases with a wide range of causes. The diseases include type 1 and type 2 diabetes, type 2 ketosis-prone diabetes (which I know exists thanks to Michael Barker’s blog), gestational diabetes, various MODY types, and various pancreatic disorders. The possible causes include genetic defects (or adaptations to very different past environments), autoimmune responses, exposure to environmental toxins, as well as viral and bacterial infections; in addition to obesity, and various other apparently unrelated factors, such as excessive growth hormone production.
Type 2 diabetes and the “tired pancreas” theory
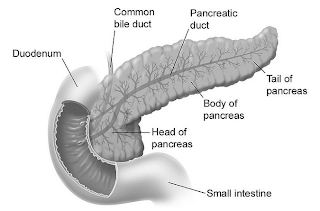
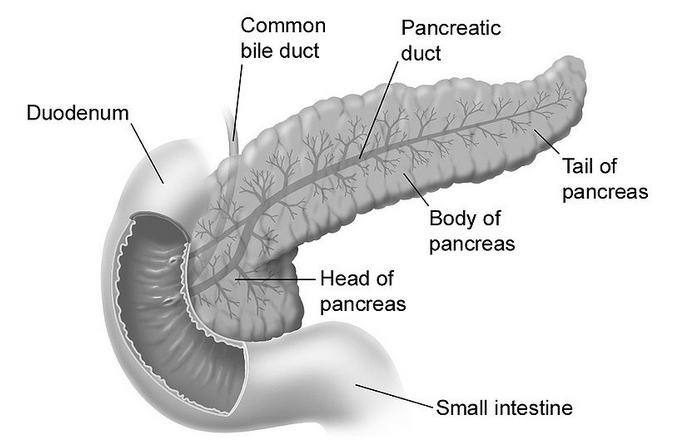
Type 2 diabetes is the one most commonly associated with the metabolic syndrome, which is characterized by middle-age central obesity, and the “diseases of civilization” brought up by Neolithic inventions. Evidence is mounting that a Neolithic diet and lifestyle play a key role in the development of the metabolic syndrome. In terms of diet, major suspects are engineered foods rich in refined carbohydrates and refined sugars. In this context, one widely touted idea is that the constant insulin spikes caused by consumption of those foods lead the pancreas (figure below from Wikipedia) to get “tired” over time, losing its ability to produce insulin. The onset of insulin resistance mediates this effect.
Empirical evidence against the “tired pancreas” theory
This “tired pancreas” theory, which refers primarily to the insulin-secreting beta-cells in the pancreas, conflicts with a lot of empirical evidence. It is inconsistent with the existence of isolated semi/full hunter-gatherer groups (e.g., the Kitavans) that consume large amounts of natural (i.e., unrefined) foods rich in easily digestible carbohydrates from tubers and fruits, which cause insulin spikes. These groups are nevertheless generally free from type 2 diabetes. The “tired pancreas” theory conflicts with the existence of isolated groups in China and Japan (e.g., the Okinawans) whose diets also include a large proportion of natural foods rich in easily digestible carbohydrates, which cause insulin spikes. Yet these groups are generally free from type 2 diabetes.
Humboldt (1995), in his personal narrative of his journey to the “equinoctial regions of the new continent”, states on page 121 about the natives as a group that: "… between twenty and fifty years old, age is not indicate by wrinkling skin, white hair or body decrepitude [among natives]. When you enter a hut is hard to differentiate a father from son …" A large proportion of these natives’ diets included plenty of natural foods rich in easily digestible carbohydrates from tubers and fruits, which cause insulin spikes. Still, there was no sign of any condition that would suggest a prevalence of type 2 diabetes among them.
At this point it is important to note that the insulin spikes caused by natural carbohydrate-rich foods are much less pronounced than the ones caused by refined carbohydrate-rich foods. The reason is that there is a huge gap between the glycemic loads of natural and refined carbohydrate-rich foods, even though the glycemic indices may be quite similar in some cases. Natural carbohydrate-rich foods are not made mostly of carbohydrates. Even an Irish (or white) potato is 75 percent water.
More insulin may lead to abnormal fat metabolism in sedentary people
The more pronounced spikes may lead to abnormal fat metabolism because more body fat is force-stored than it would have been with the less pronounced spikes, and stored body fat is not released just as promptly as it should be to fuel muscle contractions and other metabolic processes. Typically this effect is a minor one on a daily basis, but adds up over time, leading to fairly unnatural patterns of fat metabolism in the long run. This is particularly true for those who lead sedentary lifestyles. As for obesity, nobody gets obese in one day. So the key problem with the more pronounced spikes may not be that the pancreas is getting “tired”, but that body fat metabolism is not normal, which in turn leads to abnormally high or low levels of important body fat-derived hormones (e.g., high levels of leptin and low levels of adiponectin).
One common characteristic of the groups mentioned above is absence of obesity, even though food is abundant and often physical activity is moderate to low. Repeat for emphasis: “… even though food is abundant and often physical activity is moderate to low”. Note that having low levels of activity is not the same as spending the whole day sitting down in a comfortable chair working on a computer. Obviously caloric intake and level of activity among these groups were/are not at the levels that would lead to obesity. How could that be possible? See this post for a possible explanation.
Excessive body fat gain, lipotoxicity, and type 2 diabetes
There are a few theories that implicate the interaction of abnormal fat metabolism with other factors (e.g., genetic factors) in the development of type 2 diabetes. Empirical evidence suggests that this is a reasonable direction of causality. One of these theories is the theory of lipotoxicity.
Several articles have discussed the theory of lipotoxicity. The article by Unger & Zhou (2001) is a widely cited one. The theory seems to be widely based on the comparative study of various genotypes found in rats. Nevertheless, there is mounting evidence suggesting that the underlying mechanisms may be similar in humans. In a nutshell, this theory proposes the following steps in the development of type 2 diabetes:
(1) Abnormal fat mass gain leads to an abnormal increase in fat-derived hormones, of which leptin is singled out by the theory. Some people seem to be more susceptible than others in this respect, with lower triggering thresholds of fat mass gain. (What leads to exaggerated fat mass gains? The theory does not go into much detail here, but empirical evidence from other studies suggests that major culprits are refined grains and seeds, as well as refined sugars; other major culprits seem to be trans fats, and vegetable oils rich in linoleic acid.)
(2) Resistance to fat-derived hormones sets in. Again, leptin resistance is singled out as the key here. (This is a bit simplistic. Other fat-derived hormones, like adiponectin, seem to clearly interact with leptin.) Since leptin regulates fatty acid metabolism, the theory argues, leptin resistance is hypothesized to impair fatty acid metabolism.
(3) Impaired fat metabolism causes fatty acids to “spill over” to tissues other than fat cells, and also causes an abnormal increase in a substance called ceramide in those tissues. These include tissues in the pancreas that house beta-cells, which secrete insulin. In short, body fat should be stored in fat cells (adipocytes), not outside them.
(4) Initially fatty acid “spill over” to beta-cells enlarges them and makes them become overactive, leading to excessive insulin production in response to carbohydrate-rich foods, and also to insulin resistance. This is the pre-diabetic phase where hypoglycemic episodes happen a few hours following the consumption of carbohydrate-rich foods. Once this stage is reached, several natural carbohydrate-rich foods also become a problem (e.g., potatoes and bananas), in addition to refined carbohydrate-rich foods.
(5) Abnormal levels of ceramide induce beta-cell apoptosis in the pancreas. This is essentially “death by suicide” of beta cells in the pancreas. What follows is full-blown type 2 diabetes. Insulin production is impaired, leading to very elevated blood glucose levels following the consumption of carbohydrate-rich foods, even if they are unprocessed.
It is widely known that type 2 diabetics have impaired glucose metabolism. What is not so widely known is that usually they also have impaired fatty acid metabolism. For example, consumption of the same fatty meal is likely to lead to significantly more elevated triglyceride levels in type 2 diabetics than non-diabetics, after several hours. This is consistent with the notion that leptin resistance precedes type 2 diabetes, and inconsistent with the “tired pancreas” theory.
Weak and strong points of the theory of lipotoxicity
A weakness of the theory of lipotoxicity is its strong lipophobic tone; at least in the articles that I have read. See, for example, this article by Roger H. Unger in the Journal of the American Medical Association. There is ample evidence that eating a lot of the ultra-demonized saturated fat, per se, is not what makes people obese or type 2 diabetic. Yet overconsumption of trans fats and vegetable oils rich in linoleic acid does seem to be linked with obesity and type 2 diabetes. (So does the consumption of refined grains and seeds, and refined sugars.) The theory of lipotoxicity does not seem to make these distinctions.
In defense of the theory of lipotoxicity, it does not argue that there cannot be thin diabetics. Many type 1 diabetics are thin. Type 2 diabetics can also be thin, even though that is much less common. In certain individuals, the threshold of body fat gain that will precipitate lipotoxicity may be quite low. In others, the same amount of body fat gain (or more) may in fact increase their insulin sensitivity under certain circumstances – e.g., when growth hormone levels are abnormally low.
Autoimmune disorders, perhaps induced by environmental toxins, or toxins found in certain refined foods, may cause the immune system to attack the beta-cells in the pancreas. This may lead to type 1 diabetes if all beta cells are destroyed, or something that can easily be diagnosed as type 2 (or type 1.5) diabetes if only a portion of the cells are destroyed, in a way that does not involve lipotoxicity.
Nor does the theory of lipotoxicity predict that all those who become obese will develop type 2 diabetes. It only suggests that the probability will go up, particularly if other factors are present (e.g., genetic propensity). There are many people who are obese during most of their adult lives and never develop type 2 diabetes. On the other hand, some groups, like Hispanics, tend to develop type 2 diabetes more easily (often even before they reach the obese level). One only has to visit the South Texas region near the Rio Grande border to see this first hand.
What the theory proposes is a new way of understanding the development of type 2 diabetes; a way that seems to make more sense than the “tired pancreas” theory. The theory of lipitoxicity may not be entirely correct. For example, there may be other mechanisms associated with abnormal fat metabolism and consumption of Neolithic foods that cause beta-cell “suicide”, and that have nothing to do with lipotoxicity as proposed by the theory. (At least one fat-derived hormone, tumor necrosis factor-alpha, is associated with abnormal cell apoptosis when abnormally elevated. Levels of this hormone go up immediately after a meal rich in refined carbohydrates.) But the link that it proposes between obesity and type 2 diabetes seems to be right on target.
Implications and thoughts
Some implications and thoughts based on the discussion above are the following. Some are extrapolations based on the discussion in this post combined with those in other posts. At the time of this writing, there were 90 posts on this blog, in addition to many comments. See under "Labels" at the bottom-right area of this blog for a summary of topics addressed. It is hard to ignore things that were brought to light in previous posts.
- Let us start with a big one: Avoiding natural carbohydrate-rich foods in the absence of compromised glucose metabolism is unnecessary. Those foods do not “tire” the pancreas significantly more than protein-rich foods do. While carbohydrates are not essential macronutrients, protein is. In the absence of carbohydrates, protein will be used by the body to produce glucose to supply the needs of the brain and red blood cells. Protein elicits an insulin response that is comparable to that of natural carbohydrate-rich foods on a gram-adjusted basis (but significantly lower than that of refined carbohydrate-rich foods, like doughnuts and bagels). Usually protein does not lead to a measurable glucose response because glucagon is secreted together with insulin in response to ingestion of protein, preventing hypoglycemia.
- Abnormal fat gain should be used as a general measure of one’s likelihood of being “headed south” in terms of health. The “fitness” level for men and women shown on the table in this post seem like good targets for body fat percentage. The problem here, of course, is that this is not as easy as it sounds. Attempts at getting lean can lead to poor nutrition and/or starvation. These may make matters worse in some cases, leading to hormonal imbalances and uncontrollable hunger, which will eventually lead to obesity. Poor nutrition may also depress the immune system, making one susceptible to a viral or bacterial infection that may end up leading to beta-cell destruction and diabetes. A better approach is to place emphasis on eating a variety of natural foods, which are nutritious and satiating, and avoiding refined ones, which are often addictive “empty calories”. Generally fat loss should be slow to be healthy and sustainable.
- Finally, if glucose metabolism is compromised, one should avoid any foods in quantities that cause an abnormally elevated glucose or insulin response. All one needs is an inexpensive glucose meter to find out what those foods are. The following are indications of abnormally elevated glucose and insulin responses, respectively: an abnormally high glucose level 1 hour after a meal (postprandial hyperglycemia); and an abnormally low glucose level 2 to 4 hours after a meal (reactive hypoglycemia). What is abnormally high or low? Take a look at the peaks and troughs shown on the graph in this post; they should give you an idea. Some insulin resistant people using glucose meters will probably realize that they can still eat several natural carbohydrate-rich foods, but in small quantities, because those foods usually have a low glycemic load (even if their glycemic index is high).
Lucy was a vegetarian and Sapiens an omnivore. We apparently have not evolved to be pure carnivores, even though we can be if the circumstances require. But we absolutely have not evolved to eat many of the refined and industrialized foods available today, not even the ones marketed as “healthy”. Those foods do not make our pancreas “tired”. Among other things, they “mess up” fat metabolism, which may lead to type 2 diabetes through a complex process involving hormones secreted by body fat.
References
Humboldt, A.V. (1995). Personal narrative of a journey to the equinoctial regions of the new continent. New York, NY: Penguin Books.
Unger, R.H., & Zhou, Y.-T. (2001). Lipotoxicity of beta-cells in obesity and in other causes of fatty acid spillover. Diabetes, 50(1), S118-S121.
Type 2 diabetes and the “tired pancreas” theory
Type 2 diabetes is the one most commonly associated with the metabolic syndrome, which is characterized by middle-age central obesity, and the “diseases of civilization” brought up by Neolithic inventions. Evidence is mounting that a Neolithic diet and lifestyle play a key role in the development of the metabolic syndrome. In terms of diet, major suspects are engineered foods rich in refined carbohydrates and refined sugars. In this context, one widely touted idea is that the constant insulin spikes caused by consumption of those foods lead the pancreas (figure below from Wikipedia) to get “tired” over time, losing its ability to produce insulin. The onset of insulin resistance mediates this effect.
Empirical evidence against the “tired pancreas” theory
This “tired pancreas” theory, which refers primarily to the insulin-secreting beta-cells in the pancreas, conflicts with a lot of empirical evidence. It is inconsistent with the existence of isolated semi/full hunter-gatherer groups (e.g., the Kitavans) that consume large amounts of natural (i.e., unrefined) foods rich in easily digestible carbohydrates from tubers and fruits, which cause insulin spikes. These groups are nevertheless generally free from type 2 diabetes. The “tired pancreas” theory conflicts with the existence of isolated groups in China and Japan (e.g., the Okinawans) whose diets also include a large proportion of natural foods rich in easily digestible carbohydrates, which cause insulin spikes. Yet these groups are generally free from type 2 diabetes.
Humboldt (1995), in his personal narrative of his journey to the “equinoctial regions of the new continent”, states on page 121 about the natives as a group that: "… between twenty and fifty years old, age is not indicate by wrinkling skin, white hair or body decrepitude [among natives]. When you enter a hut is hard to differentiate a father from son …" A large proportion of these natives’ diets included plenty of natural foods rich in easily digestible carbohydrates from tubers and fruits, which cause insulin spikes. Still, there was no sign of any condition that would suggest a prevalence of type 2 diabetes among them.
At this point it is important to note that the insulin spikes caused by natural carbohydrate-rich foods are much less pronounced than the ones caused by refined carbohydrate-rich foods. The reason is that there is a huge gap between the glycemic loads of natural and refined carbohydrate-rich foods, even though the glycemic indices may be quite similar in some cases. Natural carbohydrate-rich foods are not made mostly of carbohydrates. Even an Irish (or white) potato is 75 percent water.
More insulin may lead to abnormal fat metabolism in sedentary people
The more pronounced spikes may lead to abnormal fat metabolism because more body fat is force-stored than it would have been with the less pronounced spikes, and stored body fat is not released just as promptly as it should be to fuel muscle contractions and other metabolic processes. Typically this effect is a minor one on a daily basis, but adds up over time, leading to fairly unnatural patterns of fat metabolism in the long run. This is particularly true for those who lead sedentary lifestyles. As for obesity, nobody gets obese in one day. So the key problem with the more pronounced spikes may not be that the pancreas is getting “tired”, but that body fat metabolism is not normal, which in turn leads to abnormally high or low levels of important body fat-derived hormones (e.g., high levels of leptin and low levels of adiponectin).
One common characteristic of the groups mentioned above is absence of obesity, even though food is abundant and often physical activity is moderate to low. Repeat for emphasis: “… even though food is abundant and often physical activity is moderate to low”. Note that having low levels of activity is not the same as spending the whole day sitting down in a comfortable chair working on a computer. Obviously caloric intake and level of activity among these groups were/are not at the levels that would lead to obesity. How could that be possible? See this post for a possible explanation.
Excessive body fat gain, lipotoxicity, and type 2 diabetes
There are a few theories that implicate the interaction of abnormal fat metabolism with other factors (e.g., genetic factors) in the development of type 2 diabetes. Empirical evidence suggests that this is a reasonable direction of causality. One of these theories is the theory of lipotoxicity.
Several articles have discussed the theory of lipotoxicity. The article by Unger & Zhou (2001) is a widely cited one. The theory seems to be widely based on the comparative study of various genotypes found in rats. Nevertheless, there is mounting evidence suggesting that the underlying mechanisms may be similar in humans. In a nutshell, this theory proposes the following steps in the development of type 2 diabetes:
(1) Abnormal fat mass gain leads to an abnormal increase in fat-derived hormones, of which leptin is singled out by the theory. Some people seem to be more susceptible than others in this respect, with lower triggering thresholds of fat mass gain. (What leads to exaggerated fat mass gains? The theory does not go into much detail here, but empirical evidence from other studies suggests that major culprits are refined grains and seeds, as well as refined sugars; other major culprits seem to be trans fats, and vegetable oils rich in linoleic acid.)
(2) Resistance to fat-derived hormones sets in. Again, leptin resistance is singled out as the key here. (This is a bit simplistic. Other fat-derived hormones, like adiponectin, seem to clearly interact with leptin.) Since leptin regulates fatty acid metabolism, the theory argues, leptin resistance is hypothesized to impair fatty acid metabolism.
(3) Impaired fat metabolism causes fatty acids to “spill over” to tissues other than fat cells, and also causes an abnormal increase in a substance called ceramide in those tissues. These include tissues in the pancreas that house beta-cells, which secrete insulin. In short, body fat should be stored in fat cells (adipocytes), not outside them.
(4) Initially fatty acid “spill over” to beta-cells enlarges them and makes them become overactive, leading to excessive insulin production in response to carbohydrate-rich foods, and also to insulin resistance. This is the pre-diabetic phase where hypoglycemic episodes happen a few hours following the consumption of carbohydrate-rich foods. Once this stage is reached, several natural carbohydrate-rich foods also become a problem (e.g., potatoes and bananas), in addition to refined carbohydrate-rich foods.
(5) Abnormal levels of ceramide induce beta-cell apoptosis in the pancreas. This is essentially “death by suicide” of beta cells in the pancreas. What follows is full-blown type 2 diabetes. Insulin production is impaired, leading to very elevated blood glucose levels following the consumption of carbohydrate-rich foods, even if they are unprocessed.
It is widely known that type 2 diabetics have impaired glucose metabolism. What is not so widely known is that usually they also have impaired fatty acid metabolism. For example, consumption of the same fatty meal is likely to lead to significantly more elevated triglyceride levels in type 2 diabetics than non-diabetics, after several hours. This is consistent with the notion that leptin resistance precedes type 2 diabetes, and inconsistent with the “tired pancreas” theory.
Weak and strong points of the theory of lipotoxicity
A weakness of the theory of lipotoxicity is its strong lipophobic tone; at least in the articles that I have read. See, for example, this article by Roger H. Unger in the Journal of the American Medical Association. There is ample evidence that eating a lot of the ultra-demonized saturated fat, per se, is not what makes people obese or type 2 diabetic. Yet overconsumption of trans fats and vegetable oils rich in linoleic acid does seem to be linked with obesity and type 2 diabetes. (So does the consumption of refined grains and seeds, and refined sugars.) The theory of lipotoxicity does not seem to make these distinctions.
In defense of the theory of lipotoxicity, it does not argue that there cannot be thin diabetics. Many type 1 diabetics are thin. Type 2 diabetics can also be thin, even though that is much less common. In certain individuals, the threshold of body fat gain that will precipitate lipotoxicity may be quite low. In others, the same amount of body fat gain (or more) may in fact increase their insulin sensitivity under certain circumstances – e.g., when growth hormone levels are abnormally low.
Autoimmune disorders, perhaps induced by environmental toxins, or toxins found in certain refined foods, may cause the immune system to attack the beta-cells in the pancreas. This may lead to type 1 diabetes if all beta cells are destroyed, or something that can easily be diagnosed as type 2 (or type 1.5) diabetes if only a portion of the cells are destroyed, in a way that does not involve lipotoxicity.
Nor does the theory of lipotoxicity predict that all those who become obese will develop type 2 diabetes. It only suggests that the probability will go up, particularly if other factors are present (e.g., genetic propensity). There are many people who are obese during most of their adult lives and never develop type 2 diabetes. On the other hand, some groups, like Hispanics, tend to develop type 2 diabetes more easily (often even before they reach the obese level). One only has to visit the South Texas region near the Rio Grande border to see this first hand.
What the theory proposes is a new way of understanding the development of type 2 diabetes; a way that seems to make more sense than the “tired pancreas” theory. The theory of lipitoxicity may not be entirely correct. For example, there may be other mechanisms associated with abnormal fat metabolism and consumption of Neolithic foods that cause beta-cell “suicide”, and that have nothing to do with lipotoxicity as proposed by the theory. (At least one fat-derived hormone, tumor necrosis factor-alpha, is associated with abnormal cell apoptosis when abnormally elevated. Levels of this hormone go up immediately after a meal rich in refined carbohydrates.) But the link that it proposes between obesity and type 2 diabetes seems to be right on target.
Implications and thoughts
Some implications and thoughts based on the discussion above are the following. Some are extrapolations based on the discussion in this post combined with those in other posts. At the time of this writing, there were 90 posts on this blog, in addition to many comments. See under "Labels" at the bottom-right area of this blog for a summary of topics addressed. It is hard to ignore things that were brought to light in previous posts.
- Let us start with a big one: Avoiding natural carbohydrate-rich foods in the absence of compromised glucose metabolism is unnecessary. Those foods do not “tire” the pancreas significantly more than protein-rich foods do. While carbohydrates are not essential macronutrients, protein is. In the absence of carbohydrates, protein will be used by the body to produce glucose to supply the needs of the brain and red blood cells. Protein elicits an insulin response that is comparable to that of natural carbohydrate-rich foods on a gram-adjusted basis (but significantly lower than that of refined carbohydrate-rich foods, like doughnuts and bagels). Usually protein does not lead to a measurable glucose response because glucagon is secreted together with insulin in response to ingestion of protein, preventing hypoglycemia.
- Abnormal fat gain should be used as a general measure of one’s likelihood of being “headed south” in terms of health. The “fitness” level for men and women shown on the table in this post seem like good targets for body fat percentage. The problem here, of course, is that this is not as easy as it sounds. Attempts at getting lean can lead to poor nutrition and/or starvation. These may make matters worse in some cases, leading to hormonal imbalances and uncontrollable hunger, which will eventually lead to obesity. Poor nutrition may also depress the immune system, making one susceptible to a viral or bacterial infection that may end up leading to beta-cell destruction and diabetes. A better approach is to place emphasis on eating a variety of natural foods, which are nutritious and satiating, and avoiding refined ones, which are often addictive “empty calories”. Generally fat loss should be slow to be healthy and sustainable.
- Finally, if glucose metabolism is compromised, one should avoid any foods in quantities that cause an abnormally elevated glucose or insulin response. All one needs is an inexpensive glucose meter to find out what those foods are. The following are indications of abnormally elevated glucose and insulin responses, respectively: an abnormally high glucose level 1 hour after a meal (postprandial hyperglycemia); and an abnormally low glucose level 2 to 4 hours after a meal (reactive hypoglycemia). What is abnormally high or low? Take a look at the peaks and troughs shown on the graph in this post; they should give you an idea. Some insulin resistant people using glucose meters will probably realize that they can still eat several natural carbohydrate-rich foods, but in small quantities, because those foods usually have a low glycemic load (even if their glycemic index is high).
Lucy was a vegetarian and Sapiens an omnivore. We apparently have not evolved to be pure carnivores, even though we can be if the circumstances require. But we absolutely have not evolved to eat many of the refined and industrialized foods available today, not even the ones marketed as “healthy”. Those foods do not make our pancreas “tired”. Among other things, they “mess up” fat metabolism, which may lead to type 2 diabetes through a complex process involving hormones secreted by body fat.
References
Humboldt, A.V. (1995). Personal narrative of a journey to the equinoctial regions of the new continent. New York, NY: Penguin Books.
Unger, R.H., & Zhou, Y.-T. (2001). Lipotoxicity of beta-cells in obesity and in other causes of fatty acid spillover. Diabetes, 50(1), S118-S121.
Thursday, August 19, 2010
The theory of supercompensation: Strength training frequency and muscle gain
Moderate strength training has a number of health benefits, and is viewed by many as an important component of a natural lifestyle that approximates that of our Stone Age ancestors. It increases bone density, muscle mass, and improves a number of health markers. Done properly, it may decrease body fat percentage.
Generally one would expect some muscle gain as a result of strength training. Men seem to be keen on upper-body gains, while women appear to prefer lower-body gains. Yet, many people do strength training for years, and experience little or no muscle gain.
Paradoxically, those people experience major strength gains, both men and women, especially in the first few months after they start a strength training program. However, those gains are due primarily to neural adaptations, and come without any significant gain in muscle mass. This can be frustrating, especially for men. Most men are after some noticeable muscle gain as a result of strength training. (Whether that is healthy is another story, especially as one gets to extremes.)
After the initial adaptation period, of “beginner” gains, typically no strength gains occur without muscle gains.
The culprits for the lack of anabolic response are often believed to be low levels of circulating testosterone and other hormones that seem to interact with testosterone to promote muscle growth, such as growth hormone. This leads many to resort to anabolic steroids, which are drugs that mimic the effects of androgenic hormones, such as testosterone. These drugs usually increase muscle mass, but have a number of negative short-term and long-term side effects.
There seems to be a better, less harmful, solution to the lack of anabolic response. Through my research on compensatory adaptation I often noticed that, under the right circumstances, people would overcompensate for obstacles posed to them. Strength training is a form of obstacle, which should generate overcompensation under the right circumstances. From a biological perspective, one would expect a similar phenomenon; a natural solution to the lack of anabolic response.
This solution is predicted by a theory that also explains a lack of anabolic response to strength training, and that unfortunately does not get enough attention outside the academic research literature. It is the theory of supercompensation, which is discussed in some detail in several high-quality college textbooks on strength training. (Unlike popular self-help books, these textbooks summarize peer-reviewed academic research, and also provide the references that are summarized.) One example is the excellent book by Zatsiorsky & Kraemer (2006) on the science and practice of strength training.
The figure below, from Zatsiorsky & Kraemer (2006), shows what happens during and after a strength training session. The level of preparedness could be seen as the load in the session, which is proportional to: the number of exercise sets, the weight lifted (or resistance overcame) in each set, and the number of repetitions in each set. The restitution period is essentially the recovery period, which must include plenty of rest and proper nutrition.
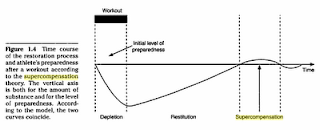
Note that toward the end there is a sideways S-like curve with a first stretch above the horizontal line and another below the line. The first stretch is the supercompensation stretch; a window in time (e.g., a 20-hour period). The horizontal line represents the baseline load, which can be seen as the baseline strength of the individual prior to the exercise session. This is where things get tricky. If one exercises again within the supercompensation stretch, strength and muscle gains will likely happen. (Usually noticeable upper-body muscle gain happens in men, because of higher levels of testosterone and of other hormones that seem to interact with testosterone.) Exercising outside the supercompensation time window may lead to no gain, or even to some loss, of both strength and muscle.
Timing strength training sessions correctly can over time lead to significant gains in strength and muscle (see middle graph in the figure below, also from Zatsiorsky & Kraemer, 2006). For that to happen, one has not only to regularly “hit” the supercompensation time window, but also progressively increase load. This must happen for each muscle group. Strength and muscle gains will occur up to a point, a point of saturation, after which no further gains are possible. Men who reach that point will invariably look muscular, in a more or less “natural” way depending on supplements and other factors. Some people seem to gain strength and muscle very easily; they are often called mesomorphs. Others are hard gainers, sometimes referred to as endomorphs (who tend to be fatter) and ectomorphs (who tend to be skinnier).

It is not easy to identify the ideal recovery and supercompensation periods. They vary from person to person. They also vary depending on types of exercise, numbers of sets, and numbers of repetitions. Nutrition also plays a role, and so do rest and stress. From an evolutionary perspective, it would seem to make sense to work all major muscle groups on the same day, and then do the same workout after a certain recovery period. (Our Stone Age ancestors did not do isolation exercises, such as bicep curls.) But this will probably make you look more like a strong hunter-gatherer than a modern bodybuilder.
To identify the supercompensation time window, one could employ a trial-and-error approach, by trying to repeat the same workout after different recovery times. Based on the literature, it would make sense to start at the 48-hour period (one full day of rest between sessions), and then move back and forth from there. A sign that one is hitting the supercompensation time window is becoming a little stronger at each workout, by performing more repetitions with the same weight (e.g., 10, from 8 in the previous session). If that happens, the weight should be incrementally increased in successive sessions. Most studies suggest that the best range for muscle gain is that of 6 to 12 repetitions in each set, but without enough time under tension gains will prove elusive.
The discussion above is not aimed at professional bodybuilders. There are a number of factors that can influence strength and muscle gain other than supercompensation. (Still, supercompensation seems to be a “biggie”.) Things get trickier over time with trained athletes, as returns on effort get progressively smaller. Even natural bodybuilders appear to benefit from different strategies at different levels of proficiency. For example, changing the workouts on a regular basis seems to be a good idea, and there is a science to doing that properly. See the “Interesting links” area of this web site for several more focused resources of strength training.
Reference:
Zatsiorsky, V., & Kraemer, W.J. (2006). Science and practice of strength training. Champaign, IL: Human Kinetics.
Generally one would expect some muscle gain as a result of strength training. Men seem to be keen on upper-body gains, while women appear to prefer lower-body gains. Yet, many people do strength training for years, and experience little or no muscle gain.
Paradoxically, those people experience major strength gains, both men and women, especially in the first few months after they start a strength training program. However, those gains are due primarily to neural adaptations, and come without any significant gain in muscle mass. This can be frustrating, especially for men. Most men are after some noticeable muscle gain as a result of strength training. (Whether that is healthy is another story, especially as one gets to extremes.)
After the initial adaptation period, of “beginner” gains, typically no strength gains occur without muscle gains.
The culprits for the lack of anabolic response are often believed to be low levels of circulating testosterone and other hormones that seem to interact with testosterone to promote muscle growth, such as growth hormone. This leads many to resort to anabolic steroids, which are drugs that mimic the effects of androgenic hormones, such as testosterone. These drugs usually increase muscle mass, but have a number of negative short-term and long-term side effects.
There seems to be a better, less harmful, solution to the lack of anabolic response. Through my research on compensatory adaptation I often noticed that, under the right circumstances, people would overcompensate for obstacles posed to them. Strength training is a form of obstacle, which should generate overcompensation under the right circumstances. From a biological perspective, one would expect a similar phenomenon; a natural solution to the lack of anabolic response.
This solution is predicted by a theory that also explains a lack of anabolic response to strength training, and that unfortunately does not get enough attention outside the academic research literature. It is the theory of supercompensation, which is discussed in some detail in several high-quality college textbooks on strength training. (Unlike popular self-help books, these textbooks summarize peer-reviewed academic research, and also provide the references that are summarized.) One example is the excellent book by Zatsiorsky & Kraemer (2006) on the science and practice of strength training.
The figure below, from Zatsiorsky & Kraemer (2006), shows what happens during and after a strength training session. The level of preparedness could be seen as the load in the session, which is proportional to: the number of exercise sets, the weight lifted (or resistance overcame) in each set, and the number of repetitions in each set. The restitution period is essentially the recovery period, which must include plenty of rest and proper nutrition.

Note that toward the end there is a sideways S-like curve with a first stretch above the horizontal line and another below the line. The first stretch is the supercompensation stretch; a window in time (e.g., a 20-hour period). The horizontal line represents the baseline load, which can be seen as the baseline strength of the individual prior to the exercise session. This is where things get tricky. If one exercises again within the supercompensation stretch, strength and muscle gains will likely happen. (Usually noticeable upper-body muscle gain happens in men, because of higher levels of testosterone and of other hormones that seem to interact with testosterone.) Exercising outside the supercompensation time window may lead to no gain, or even to some loss, of both strength and muscle.
Timing strength training sessions correctly can over time lead to significant gains in strength and muscle (see middle graph in the figure below, also from Zatsiorsky & Kraemer, 2006). For that to happen, one has not only to regularly “hit” the supercompensation time window, but also progressively increase load. This must happen for each muscle group. Strength and muscle gains will occur up to a point, a point of saturation, after which no further gains are possible. Men who reach that point will invariably look muscular, in a more or less “natural” way depending on supplements and other factors. Some people seem to gain strength and muscle very easily; they are often called mesomorphs. Others are hard gainers, sometimes referred to as endomorphs (who tend to be fatter) and ectomorphs (who tend to be skinnier).

It is not easy to identify the ideal recovery and supercompensation periods. They vary from person to person. They also vary depending on types of exercise, numbers of sets, and numbers of repetitions. Nutrition also plays a role, and so do rest and stress. From an evolutionary perspective, it would seem to make sense to work all major muscle groups on the same day, and then do the same workout after a certain recovery period. (Our Stone Age ancestors did not do isolation exercises, such as bicep curls.) But this will probably make you look more like a strong hunter-gatherer than a modern bodybuilder.
To identify the supercompensation time window, one could employ a trial-and-error approach, by trying to repeat the same workout after different recovery times. Based on the literature, it would make sense to start at the 48-hour period (one full day of rest between sessions), and then move back and forth from there. A sign that one is hitting the supercompensation time window is becoming a little stronger at each workout, by performing more repetitions with the same weight (e.g., 10, from 8 in the previous session). If that happens, the weight should be incrementally increased in successive sessions. Most studies suggest that the best range for muscle gain is that of 6 to 12 repetitions in each set, but without enough time under tension gains will prove elusive.
The discussion above is not aimed at professional bodybuilders. There are a number of factors that can influence strength and muscle gain other than supercompensation. (Still, supercompensation seems to be a “biggie”.) Things get trickier over time with trained athletes, as returns on effort get progressively smaller. Even natural bodybuilders appear to benefit from different strategies at different levels of proficiency. For example, changing the workouts on a regular basis seems to be a good idea, and there is a science to doing that properly. See the “Interesting links” area of this web site for several more focused resources of strength training.
Reference:
Zatsiorsky, V., & Kraemer, W.J. (2006). Science and practice of strength training. Champaign, IL: Human Kinetics.
What can beetles tell us about slowing aging? Answers are in the mitochondria
 |
| Mitochondrial genes influence life expectancy in beetles, a new study reports. |
The mitochondria—kidney-shaped organelles often referred to as the cell's powerhouses—each contain their own set of DNA, passed on from mother to offspring, and according to the study, it's these strands that may hold key genes that determine one's life expectancy, at least in bugs.
The study, published in the August issue of The American Naturalist, found evidence that particular combinations of genes (haplotypes) in the mitochondrial genome influenced lifespan in a species of seed beetles (Callosobruchus maculates).
As a result, the research supports growing evidence that particular mitochondrial gene combinations could also play a major role in accelerating the aging process in humans because they could cause mitochondria to produce greater amounts of toxic molecules called free radicals causing oxidative damage to cells, cellular proteins and DNA.
Evolutionary biologist Damian Dowling of Melbourne, who conducted the study, hopes his research will help medical scientists identify which gene combinations accelerate aging, as well as develop gene therapies that alter the combinations, or develop antioxidant therapies that neutralize free radicals and protect cells from oxidative damage. Do mothers show favoritism toward daughters?
Although Dowling found his discovery interesting, he said it was not the original intent of his research; in fact, he was testing a debated theory that mitochondrial genes make an impact on the tug-of-war between the sexes in the beetles. Previous research in beetles and fruit flies has explored a ubiquitous phenomenon in insects commonly called the "cost of mating"—that is, that the simple act of sexual reproduction can take a toll on mothers, and sometimes fathers, by reducing their life expectancy.
Dowling’s wanted to find out if mitochondria bestowed any reward to female beetles. He explained to me: "Because the mitochondrial genome is maternally inherited it has been hypothesized that it will take the female's best interests at heart."
But, he adds, "Our study was the first experimental test of this idea, and we didn't support the controversial idea." However, what Dowling did find was something more exciting—that different mitochondrial gene combinations, sourced from different geographic locations from around the globe, produced large differences in life spans in the beetles.
“Beetles that harbored certain mitochondrial DNA sequences could live up to 30 percent longer,” he told me. Thirty percent longer is about 20 more days for the life of a beetle, which is nothing short of a leap for the crawling critters—when scaled up to human years, it amounts to adding about 23 more years.
Tuesday, August 17, 2010
How to win her heart? Moderate amounts of dark chocolate
They say chocolate is the way to a woman's heart, and they could be right – eating one or two servings of dark chocolate weekly is good for the hearts of middle-aged or elderly women.
A nine-year observational study followed 31,823 healthy Swedish women ages 48 to 82 and found that those who ate moderate amounts of high-quality chocolate had healthier hearts.
The women who gained the most heart-health benefits had eaten one or two servings of the dark chocolate weekly, followed by those who ate one to three servings monthly. Each serving of chocolate was typically between 19 and 30 grams.
On the other hand, the women who ate one or more servings per day received no benefit, which the researchers suggest was result of replacing other nutritious foods with the chocolate. So, enjoy dark chocolate, but in moderation and as part of a nutritious diet.
Men, take note – the quality of the chocolate matters.
Finding the right chocolate for a woman’s heart health, while avoiding the pitfalls of eating other chocolates high in fat and sugar, depends on content and value of its cocoa.
The chocolate the Swedish women ate contained higher amounts of cocoa than milk chocolate and was not as highly processed as most dark chocolate found typically in North America.
When choosing dark chocolate, seek out versions that are minimally processed and high in cocoa flavonoids for greatest antioxidant strength. Cocoa is naturally one of the world's richest sources of antioxidant flavonoids, which are also found in various fruits and vegetables, tea and red wine.
Previous studies have explored dark chocolate as a delicious and convenient way to gain sufficient antioxidants to support cell health, cardiovascular and heart health.
Source: Mostofsky E., Levitan E.B., Wolk A. et al. Journal of the American Heart Association.
Note: This original post was written to be published here.
A nine-year observational study followed 31,823 healthy Swedish women ages 48 to 82 and found that those who ate moderate amounts of high-quality chocolate had healthier hearts.
The women who gained the most heart-health benefits had eaten one or two servings of the dark chocolate weekly, followed by those who ate one to three servings monthly. Each serving of chocolate was typically between 19 and 30 grams.
On the other hand, the women who ate one or more servings per day received no benefit, which the researchers suggest was result of replacing other nutritious foods with the chocolate. So, enjoy dark chocolate, but in moderation and as part of a nutritious diet.
Men, take note – the quality of the chocolate matters.
Finding the right chocolate for a woman’s heart health, while avoiding the pitfalls of eating other chocolates high in fat and sugar, depends on content and value of its cocoa.
The chocolate the Swedish women ate contained higher amounts of cocoa than milk chocolate and was not as highly processed as most dark chocolate found typically in North America.
When choosing dark chocolate, seek out versions that are minimally processed and high in cocoa flavonoids for greatest antioxidant strength. Cocoa is naturally one of the world's richest sources of antioxidant flavonoids, which are also found in various fruits and vegetables, tea and red wine.
Previous studies have explored dark chocolate as a delicious and convenient way to gain sufficient antioxidants to support cell health, cardiovascular and heart health.
Source: Mostofsky E., Levitan E.B., Wolk A. et al. Journal of the American Heart Association.
Note: This original post was written to be published here.
Friday, August 13, 2010
The evolution of costly traits: Competing for women can be unhealthy for men
There are human traits that evolved in spite of being survival handicaps. These counterintuitive traits are often called costly traits, or Zahavian traits (in animal signaling contexts), in honor of the evolutionary biologist Amotz Zahavi (Zahavi & Zahavi, 1997). I have written a post about this type of traits, and also an academic article (Kock, 2009). The full references and links to these publications are at the end of this post.
The classic example of costly trait is the peacock’s train, which is used by males to signal health to females. (Figure below from: animals.howstuffworks.com.) The male peacock’s train (often incorrectly called “tail”) is a costly trait because it impairs the ability of a male to flee predators. It decreases a male’s survival success, even though it has a positive net effect on the male’s reproductive success (i.e., the number of offspring it generates). It is used in sexual selection; the females find big and brightly colored trains with many eye spots "sexy".
So costly traits exist in many species, including the human species, but we have not identified them all yet. The implication for human diet and lifestyle choices is that our ancestors might have evolved some habits that are bad for human survival, and moved away from others that are good for survival. And I am not only talking about survival among modern humans; I am talking about survival among our human ancestors too.
The simple reason for the existence of costly traits in humans is that evolution tends to maximize reproductive success, not survival, and that applies to all species. (Inclusive fitness theory goes a step further, placing the gene at the center of the selection process, but this is a topic for another post.) If that were not the case, rodent species, as well as other species that specialize in fast reproduction within relatively short life spans, would never have evolved.
Here is an interesting piece of news about research done at the University of Michigan. (I have met the lead researcher, Dan Kruger, a couple of times at HBES conferences. My impression is that his research is solid.) The research illustrates the evolution of costly traits, from a different angle. The researchers argue, based on the results of their investigation, that competing for a woman’s attention is generally bad for a man’s health!
Very romantic ...
References:
Kock, N. (2009). The evolution of costly traits through selection and the importance of oral speech in e-collaboration. Electronic Markets, 19(4), 221-232.
Zahavi, A. & Zahavi, A. (1997). The Handicap Principle: A missing piece of Darwin’s puzzle. Oxford, England: Oxford University Press.
The classic example of costly trait is the peacock’s train, which is used by males to signal health to females. (Figure below from: animals.howstuffworks.com.) The male peacock’s train (often incorrectly called “tail”) is a costly trait because it impairs the ability of a male to flee predators. It decreases a male’s survival success, even though it has a positive net effect on the male’s reproductive success (i.e., the number of offspring it generates). It is used in sexual selection; the females find big and brightly colored trains with many eye spots "sexy".

So costly traits exist in many species, including the human species, but we have not identified them all yet. The implication for human diet and lifestyle choices is that our ancestors might have evolved some habits that are bad for human survival, and moved away from others that are good for survival. And I am not only talking about survival among modern humans; I am talking about survival among our human ancestors too.
The simple reason for the existence of costly traits in humans is that evolution tends to maximize reproductive success, not survival, and that applies to all species. (Inclusive fitness theory goes a step further, placing the gene at the center of the selection process, but this is a topic for another post.) If that were not the case, rodent species, as well as other species that specialize in fast reproduction within relatively short life spans, would never have evolved.
Here is an interesting piece of news about research done at the University of Michigan. (I have met the lead researcher, Dan Kruger, a couple of times at HBES conferences. My impression is that his research is solid.) The research illustrates the evolution of costly traits, from a different angle. The researchers argue, based on the results of their investigation, that competing for a woman’s attention is generally bad for a man’s health!
Very romantic ...
References:
Kock, N. (2009). The evolution of costly traits through selection and the importance of oral speech in e-collaboration. Electronic Markets, 19(4), 221-232.
Zahavi, A. & Zahavi, A. (1997). The Handicap Principle: A missing piece of Darwin’s puzzle. Oxford, England: Oxford University Press.
Wednesday, August 11, 2010
Resveratrol-Rich Plant Extract Stifles Inflammation in Humans
Resveratrol’s antioxidant and anti-inflammation actions shown previously only in vitro and in laboratory animals have now been observed in a small human study.
State University of Buffalo New York and Kaleida Health researchers found that supplementation with a plant extract containing resveratrol suppressed generation of free radicals called reactive oxygen species (ROS) and reduced expression of two major proinflammatory pathways.
Writing in their study, published in Journal of Clinical Endocrinology and Metabolism, the researchers state that they have demonstrated for the first time in humans “comprehensive effects on ROS generation and inflammation” and the “antiaging action of resveratrol.”
In the trial, two groups of 10 healthy adults were randomized to receive placebo or 200 milligrams of Japanese knotweed extract (Polygonum cuspidatum) supplying 40 milligrams of resveratrol daily. Fasting blood samples were collected before, during and after six weeks of supplementation. Subjects chosen were not on any antiinflammatory drugs.
The researchers’ data showed clear suppression of ROS generation and reduced expression of TNF-alpha and IL-6, which are regulated by NFkB, that led to falling levels of C-reactive protein, which are all involved with inflammatory response.
In parallel, the extract reduced expression of two major proinflammatory enzymes, JNK-1 and IKK-beta.
Resveratrol’s effects on reducing oxidative stress and inflammation are thought to take place because it activates production of SIRT1, one of a family of proteins that is positively associated with influencing fat metabolism, slowing aging, and extending lifespan in response to calorie restriction and fasting in yeast and animals.
Chronic oxidative stress and inflammation are implicated as factors that accelerate aging because of damage caused to cellular components including membranes, mitochondria and DNA.
Source: Ghanim H, Sia CL, Abuaysheh S, Korzeniewski K, Patnaik P, Marumganti A, Chaudhuri A, Dandona P. An Antiinflammatory and Reactive oxygen Species Suprressive Effects of an Extract of Polygonum Cuspidatum Containing Resveratrol. J Clin Endocrin Metab. 2010; 10:12.
State University of Buffalo New York and Kaleida Health researchers found that supplementation with a plant extract containing resveratrol suppressed generation of free radicals called reactive oxygen species (ROS) and reduced expression of two major proinflammatory pathways.
Writing in their study, published in Journal of Clinical Endocrinology and Metabolism, the researchers state that they have demonstrated for the first time in humans “comprehensive effects on ROS generation and inflammation” and the “antiaging action of resveratrol.”
In the trial, two groups of 10 healthy adults were randomized to receive placebo or 200 milligrams of Japanese knotweed extract (Polygonum cuspidatum) supplying 40 milligrams of resveratrol daily. Fasting blood samples were collected before, during and after six weeks of supplementation. Subjects chosen were not on any antiinflammatory drugs.
The researchers’ data showed clear suppression of ROS generation and reduced expression of TNF-alpha and IL-6, which are regulated by NFkB, that led to falling levels of C-reactive protein, which are all involved with inflammatory response.
In parallel, the extract reduced expression of two major proinflammatory enzymes, JNK-1 and IKK-beta.
Resveratrol’s effects on reducing oxidative stress and inflammation are thought to take place because it activates production of SIRT1, one of a family of proteins that is positively associated with influencing fat metabolism, slowing aging, and extending lifespan in response to calorie restriction and fasting in yeast and animals.
Chronic oxidative stress and inflammation are implicated as factors that accelerate aging because of damage caused to cellular components including membranes, mitochondria and DNA.
Source: Ghanim H, Sia CL, Abuaysheh S, Korzeniewski K, Patnaik P, Marumganti A, Chaudhuri A, Dandona P. An Antiinflammatory and Reactive oxygen Species Suprressive Effects of an Extract of Polygonum Cuspidatum Containing Resveratrol. J Clin Endocrin Metab. 2010; 10:12.
Tuesday, August 10, 2010
Nonexercise activities like fidgeting may account for a 1,000 percent difference in body fat gain! NEAT eh?
Some studies become classics in their fields and yet are largely missed by the popular media. This seems to be what happened with a study by Levine and colleagues (1999; full reference and link at the end of this post), which looked at the role that nonexercise activity thermogenesis (NEAT) plays in fat gain suppression. Many thanks go to Lyle McDonald for posting on this.
You have probably seen on the web claims that overeating leads to fat loss, because overeating increases one’s basal metabolic rate. There are also claims that food has a powerful thermic effect, due to the energy needed for digestion, absorption and storage of nutrients; this is also claimed to lead to fat loss. There is some truth to these claims, but the related effects are very small compared with the effects of NEAT.
Ever wonder why there are some folks who seem to eat whatever they want, and never get fat? As it turns out, it may be primarily due to NEAT!
NEAT is associated with fidgeting, maintenance of posture, shifting position, pacing, and other involuntary light physical activities. The main finding of this study was that NEAT accounted for a massive amount of the difference in body fat gain among the participants in the study. The participants were 12 males and 4 females, ranging in age from 25 to 36 years. These healthy and lean participants were fed 1,000 kilocalories per day in excess of their weight-maintenance requirements, for a period of 8 weeks. See figure below; click on it to enlarge.
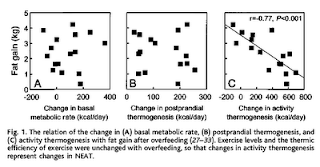
Fat gain varied more than 10-fold among the participants (or more than 1,000 percent), ranging from a gain of only 0.36 kg (0.79 lbs) to a gain of 4.23 kg (9.33 lbs). As you can see, NEAT explains a lot of the variance in the fat gain variable, which is indicated by the highly statistically significant negative correlation (-0.77). Its effect dwarfs those related to basal metabolic rate and food-induced thermogenesis, neither of which was statistically significant.
How can one use this finding in practice? This research indirectly suggests that moving often throughout the day may have a significant additive long term effect on fat gain suppression. It is reasonable to expect a similar effect on fat loss. And this effect may be stealthy enough to prevent the body from reacting to fat loss by significantly lowering its basal metabolic rate. (Yes, while the increase in basal metabolic rate is trivial in response to overfeeding, the decrease in this rate is nontrivial in response to underfeeding. Essentially the body is much more “concerned” about starving than fattening up.)
The bad news is that it is not easy to mimic the effects of NEAT through voluntary activities. The authors of the study estimated that the maximum increase in NEAT detected in the study (692 kcal/day) would be equivalent to a 15-minute walk every waking hour of every single day! (This other study focuses specifically on fidgeting.) Clearly NEAT has a powerful effect on weight loss, which is not easy to match with voluntary pacing, standing up etc. Moreover, females seem to benefit less from NEAT, because they seem to engage in fewer NEAT-related activities than men. The four lowest NEAT values in the study corresponded to the four female participants.
Nevertheless, if you have a desk job, like I do, you may want to stand up and pace for a few seconds every 30 minutes. You may also want to stand up while you talk on the phone. You may want to shift position from time to time; e.g., sitting at the edge of the chair for a few minutes every hour, without back support. And so on. These actions may take you a bit closer to the lifestyle of our Paleolithic ancestors, who were not sitting down motionless the whole day. Try also eating more like they did and, over a year, the results may be dramatic!
Reference:
James A. Levine, Norman L. Eberhardt, Michael D. Jensen (1999). Role of nonexercise activity thermogenesis in resistance to fat gain in humans. Science, 283(5399), 212-214.
You have probably seen on the web claims that overeating leads to fat loss, because overeating increases one’s basal metabolic rate. There are also claims that food has a powerful thermic effect, due to the energy needed for digestion, absorption and storage of nutrients; this is also claimed to lead to fat loss. There is some truth to these claims, but the related effects are very small compared with the effects of NEAT.
Ever wonder why there are some folks who seem to eat whatever they want, and never get fat? As it turns out, it may be primarily due to NEAT!
NEAT is associated with fidgeting, maintenance of posture, shifting position, pacing, and other involuntary light physical activities. The main finding of this study was that NEAT accounted for a massive amount of the difference in body fat gain among the participants in the study. The participants were 12 males and 4 females, ranging in age from 25 to 36 years. These healthy and lean participants were fed 1,000 kilocalories per day in excess of their weight-maintenance requirements, for a period of 8 weeks. See figure below; click on it to enlarge.

Fat gain varied more than 10-fold among the participants (or more than 1,000 percent), ranging from a gain of only 0.36 kg (0.79 lbs) to a gain of 4.23 kg (9.33 lbs). As you can see, NEAT explains a lot of the variance in the fat gain variable, which is indicated by the highly statistically significant negative correlation (-0.77). Its effect dwarfs those related to basal metabolic rate and food-induced thermogenesis, neither of which was statistically significant.
How can one use this finding in practice? This research indirectly suggests that moving often throughout the day may have a significant additive long term effect on fat gain suppression. It is reasonable to expect a similar effect on fat loss. And this effect may be stealthy enough to prevent the body from reacting to fat loss by significantly lowering its basal metabolic rate. (Yes, while the increase in basal metabolic rate is trivial in response to overfeeding, the decrease in this rate is nontrivial in response to underfeeding. Essentially the body is much more “concerned” about starving than fattening up.)
The bad news is that it is not easy to mimic the effects of NEAT through voluntary activities. The authors of the study estimated that the maximum increase in NEAT detected in the study (692 kcal/day) would be equivalent to a 15-minute walk every waking hour of every single day! (This other study focuses specifically on fidgeting.) Clearly NEAT has a powerful effect on weight loss, which is not easy to match with voluntary pacing, standing up etc. Moreover, females seem to benefit less from NEAT, because they seem to engage in fewer NEAT-related activities than men. The four lowest NEAT values in the study corresponded to the four female participants.
Nevertheless, if you have a desk job, like I do, you may want to stand up and pace for a few seconds every 30 minutes. You may also want to stand up while you talk on the phone. You may want to shift position from time to time; e.g., sitting at the edge of the chair for a few minutes every hour, without back support. And so on. These actions may take you a bit closer to the lifestyle of our Paleolithic ancestors, who were not sitting down motionless the whole day. Try also eating more like they did and, over a year, the results may be dramatic!
Reference:
James A. Levine, Norman L. Eberhardt, Michael D. Jensen (1999). Role of nonexercise activity thermogenesis in resistance to fat gain in humans. Science, 283(5399), 212-214.
Saturday, August 7, 2010
Cortisol, surprise-enhanced cognition, and flashbulb memories: Scaring people with a snake screen and getting a PhD for it!
Cortisol is a hormone that has a number of important functions. It gets us out of bed in the morning, it cranks up our metabolism in preparation for intense exercise, and it also helps us memorize things and even learn. Yes, it helps us learn. Memorization in particular, and cognition in general, would be significantly impaired without cortisol. When you are surprised, particularly with something unpleasant, cortisol levels increase and enhance cognition. This is in part what an interesting study suggests; a study in which I was involved. The study was properly “sanctified” by the academic peer-review process (Kock et al., 2009; full reference and link at the end of this post).
The main hypothesis tested through this study is also known as the “flashbulb memorization” hypothesis. Interestingly, up until this study was conducted no one seemed to have used evolution to provide a basis on which flashbulb memorization can be explained. The basic idea here is that enhanced cognition within the temporal vicinity of animal attacks (i.e., a few minutes before and after) allowed our hominid ancestors to better build and associate memories related to the animals and their typical habitat markers (e.g., vegetation, terrain, rock formations), which in turn increased their survival chances. Their survival chances increased because the memories helped them avoid a second encounter; if they survived the first, of course. And so flashbulb memorization evolved. (In fact, it might have evolved earlier than at the hominid stage, and it may also have evolved in other species.)
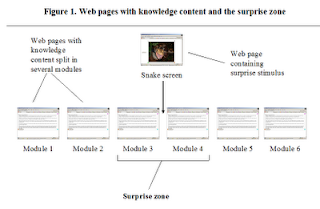
The study involved 186 student participants. The participants were asked to review web-based learning modules and subsequently take a test on what they had learned. Data from 6 learning modules in 2 experimental conditions were contrasted. In the treatment condition a web-based screen with a snake in attack position was used to surprise the participants; the snake screen was absent in the control condition. See schematic figure below (click on it to enlarge). The “surprise zone” in the figure comprises the modules immediately before and after the snake screen (modules 3 and 4); those are the modules in which higher scores were predicted.
The figure below (click on it to enlarge) shows a summary of the results. The top part of the figure shows the percentage differences between average scores obtained by participants in the treatment and control conditions. The bottom part of the figure shows the average scores obtained by participants in both conditions, as well as the scores that the participants would have obtained by chance. The chance scores would likely have been the ones obtained by the participants if their learning had been significantly impaired for any of the modules; this could have happened due to distraction, for example. As you can see, the scores for all modules are significantly higher than chance.

In summary, the participants who were surprised with the snake screen obtained significantly higher scores for the two modules immediately before (about 20 percent higher) and after (about 40 percent higher) the snake screen. The reason is that the surprise elicited by the snake screen increased cortisol levels, which in turn improved learning for modules 3 and 4. Adrenaline and noradrenaline (epinephrine and norepinephrine) may also be involved. This phenomenon is so odd that it seems to defy the laws of physics; note that Module 3 was reviewed before the snake screen. And, depending on the size of a test, this could have turned a “C” into an “A” grade!
Similarly, it is because of this action of cortisol that Americans reading this post, especially those who lived in the East Coast in 2001, remember vividly where they were, what they were doing, and who they were with, when they first heard about the September 11, 2001 Attacks. I was living in Philadelphia at the time, and I remember those details very vividly, even though the Attacks happened almost 10 years ago. That is one of the fascinating things that cortisol does; it instantaneously turns short-term contextual memories temporally associated with a surprise event (i.e., a few minutes before and after the event) into vivid long-term memories.
This study was part of the PhD research project of one of my former doctoral students, and now Dr. Ruth Chatelain-Jardon. Her PhD was granted in May 2010. She expanded the study through data collection in two different countries, and a wide range of analyses. (It is not that easy to get a PhD!) Her research provides solid evidence that flashbulb memorization is a real phenomenon, and also that it is a human universal. Thanks are also due to Dr. Jesus Carmona, another former doctoral student of mine who worked on a different PhD research project, but who also helped a lot with this project.
Reference:
Kock, N., Chatelain-Jardón, R., & Carmona, J. (2009). Scaring them into learning!? Using a snake screen to enhance the knowledge transfer effectiveness of a web interface. Decision Sciences Journal of Innovative Education, 7(2), 359-375.
The main hypothesis tested through this study is also known as the “flashbulb memorization” hypothesis. Interestingly, up until this study was conducted no one seemed to have used evolution to provide a basis on which flashbulb memorization can be explained. The basic idea here is that enhanced cognition within the temporal vicinity of animal attacks (i.e., a few minutes before and after) allowed our hominid ancestors to better build and associate memories related to the animals and their typical habitat markers (e.g., vegetation, terrain, rock formations), which in turn increased their survival chances. Their survival chances increased because the memories helped them avoid a second encounter; if they survived the first, of course. And so flashbulb memorization evolved. (In fact, it might have evolved earlier than at the hominid stage, and it may also have evolved in other species.)
The study involved 186 student participants. The participants were asked to review web-based learning modules and subsequently take a test on what they had learned. Data from 6 learning modules in 2 experimental conditions were contrasted. In the treatment condition a web-based screen with a snake in attack position was used to surprise the participants; the snake screen was absent in the control condition. See schematic figure below (click on it to enlarge). The “surprise zone” in the figure comprises the modules immediately before and after the snake screen (modules 3 and 4); those are the modules in which higher scores were predicted.

The figure below (click on it to enlarge) shows a summary of the results. The top part of the figure shows the percentage differences between average scores obtained by participants in the treatment and control conditions. The bottom part of the figure shows the average scores obtained by participants in both conditions, as well as the scores that the participants would have obtained by chance. The chance scores would likely have been the ones obtained by the participants if their learning had been significantly impaired for any of the modules; this could have happened due to distraction, for example. As you can see, the scores for all modules are significantly higher than chance.

In summary, the participants who were surprised with the snake screen obtained significantly higher scores for the two modules immediately before (about 20 percent higher) and after (about 40 percent higher) the snake screen. The reason is that the surprise elicited by the snake screen increased cortisol levels, which in turn improved learning for modules 3 and 4. Adrenaline and noradrenaline (epinephrine and norepinephrine) may also be involved. This phenomenon is so odd that it seems to defy the laws of physics; note that Module 3 was reviewed before the snake screen. And, depending on the size of a test, this could have turned a “C” into an “A” grade!
Similarly, it is because of this action of cortisol that Americans reading this post, especially those who lived in the East Coast in 2001, remember vividly where they were, what they were doing, and who they were with, when they first heard about the September 11, 2001 Attacks. I was living in Philadelphia at the time, and I remember those details very vividly, even though the Attacks happened almost 10 years ago. That is one of the fascinating things that cortisol does; it instantaneously turns short-term contextual memories temporally associated with a surprise event (i.e., a few minutes before and after the event) into vivid long-term memories.
This study was part of the PhD research project of one of my former doctoral students, and now Dr. Ruth Chatelain-Jardon. Her PhD was granted in May 2010. She expanded the study through data collection in two different countries, and a wide range of analyses. (It is not that easy to get a PhD!) Her research provides solid evidence that flashbulb memorization is a real phenomenon, and also that it is a human universal. Thanks are also due to Dr. Jesus Carmona, another former doctoral student of mine who worked on a different PhD research project, but who also helped a lot with this project.
Reference:
Kock, N., Chatelain-Jardón, R., & Carmona, J. (2009). Scaring them into learning!? Using a snake screen to enhance the knowledge transfer effectiveness of a web interface. Decision Sciences Journal of Innovative Education, 7(2), 359-375.
Friday, August 6, 2010
David Cameron's Big Society as a 'word cloud' with thanks to wordle.net
 |
| David Cameron's speech on Big Society presented as a 'word cloud'... (...does this look like a shark?) |
Wednesday, August 4, 2010
The baffling rise in seasonal allergies: Global warming or obesity?
The July 26, 2010 issue of Fortune has an interesting set of graphs on page 14. It shows the rise of allergies in the USA, together with figures on lost productivity, doctor visits, and medical expenditures. (What would you expect? This is Fortune, and money matters.) It also shows some cool maps with allergen concentrations, and how they are likely to increase with global warming. (See below; click on it to enlarge; use the "CRTL" and "+" keys to zoom in, and CRTL" and "-" to zoom out.)
The implication: A rise in global temperatures is causing an increase in allergy cases. Supposedly the spring season starts earlier, with more pollen being produced overall, and thus more allergy cases.
Really!?
I checked their numbers against population growth, because as the population of a country increases, so will the absolute number of allergy cases (as well as cancer cases, and cases of almost any disease). What is important is whether there has been an increase in allergy rates, or the percentage of the population suffering from allergies. Well, indeed, allergy rates have been increasing.
Now, I don’t know about your neck of the woods, but temperatures have been unusually low this year in South Texas. Global warming may be happening, but given recent fluctuations in temperature, I am not sure global warming explains the increases in allergy rates. Particularly the spike in allergy rates in 2010; this seems to be very unlikely to be caused by global warming.
And I have my own experience of going from looking like a seal to looking more like a human being. When I was a seal (i.e., looked like one), I used to have horrible seasonal pollen allergies. Then I lost 60 lbs, and my allergies diminished dramatically. Why? Body fat secretes a number of pro-inflammatory hormones (see, e.g., this post, and also this one), and allergies are essentially exaggerated inflammatory responses.
So I added obesity rates to the mix, and came up with the table and graph below (click on it to enlarge).
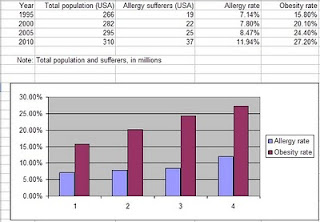
Obesity rates and allergies do seem to go hand in hand, don’t you think? The correlation between obesity and allergy rates is a high 0.87!
Assuming that this correlation reflects reasonably well the relationship between obesity and allergy rates (something that is not entirely clear given the small sample), obesity would still explain only 75.7 percent of the variance in allergy rates (this number is the correlation squared). That is, about 24.3 percent of the variance in allergy rates would be due to other missing factors.
A strong candidate for missing factor is something that makes people obese in the first place, namely consumption of foods rich in refined grains, seeds, and sugars. Again, in my experience, removing these foods from my diet reduced the intensity of allergic reactions, but not as much as losing a significant amount of body fat. We are talking about things like cereals, white bread, doughnuts, pasta, pancakes covered with syrup, regular sodas, and fruit juices. Why? These foods also seem to increase serum concentrations of pro-inflammatory hormones within hours of their consumption.
Other candidates are vitamin D levels, and lack of exposure to natural environments during childhood, just to name a few. People seem to avoid the sun like the plague these days, which can lower their vitamin D levels. This is a problem because vitamin D modulates immune responses; so it is important in the spring, as well as in the winter. The lack of exposure to natural environments during childhood may make people more sensitive to natural allergens, like pollen.

The implication: A rise in global temperatures is causing an increase in allergy cases. Supposedly the spring season starts earlier, with more pollen being produced overall, and thus more allergy cases.
Really!?
I checked their numbers against population growth, because as the population of a country increases, so will the absolute number of allergy cases (as well as cancer cases, and cases of almost any disease). What is important is whether there has been an increase in allergy rates, or the percentage of the population suffering from allergies. Well, indeed, allergy rates have been increasing.
Now, I don’t know about your neck of the woods, but temperatures have been unusually low this year in South Texas. Global warming may be happening, but given recent fluctuations in temperature, I am not sure global warming explains the increases in allergy rates. Particularly the spike in allergy rates in 2010; this seems to be very unlikely to be caused by global warming.
And I have my own experience of going from looking like a seal to looking more like a human being. When I was a seal (i.e., looked like one), I used to have horrible seasonal pollen allergies. Then I lost 60 lbs, and my allergies diminished dramatically. Why? Body fat secretes a number of pro-inflammatory hormones (see, e.g., this post, and also this one), and allergies are essentially exaggerated inflammatory responses.
So I added obesity rates to the mix, and came up with the table and graph below (click on it to enlarge).

Obesity rates and allergies do seem to go hand in hand, don’t you think? The correlation between obesity and allergy rates is a high 0.87!
Assuming that this correlation reflects reasonably well the relationship between obesity and allergy rates (something that is not entirely clear given the small sample), obesity would still explain only 75.7 percent of the variance in allergy rates (this number is the correlation squared). That is, about 24.3 percent of the variance in allergy rates would be due to other missing factors.
A strong candidate for missing factor is something that makes people obese in the first place, namely consumption of foods rich in refined grains, seeds, and sugars. Again, in my experience, removing these foods from my diet reduced the intensity of allergic reactions, but not as much as losing a significant amount of body fat. We are talking about things like cereals, white bread, doughnuts, pasta, pancakes covered with syrup, regular sodas, and fruit juices. Why? These foods also seem to increase serum concentrations of pro-inflammatory hormones within hours of their consumption.
Other candidates are vitamin D levels, and lack of exposure to natural environments during childhood, just to name a few. People seem to avoid the sun like the plague these days, which can lower their vitamin D levels. This is a problem because vitamin D modulates immune responses; so it is important in the spring, as well as in the winter. The lack of exposure to natural environments during childhood may make people more sensitive to natural allergens, like pollen.
Sunday, August 1, 2010
BIG SOCIETY: Arts, Health and Well-Being
Hello and a big THANK YOU to everyone who’s taken part in discussions around the Lib-Con Big Society over the last 3 weeks. In Barnsley, Bolton, Ellesmere Port and Manchester, we’ve had some really interesting exchanges.
The last North West Arts and Health Networking Event was one of the most stimulating and animated discussions with lots of thoughts about inclusion, subversion and action, and I can’t begin to reflect your contributions here. I know people are apprehensive about committing their thoughts to a blog, but it’s all good and keeps conversation flowing. Of course, if I can’t persuade you to write anything here, please feel free to carry on emailing me.
 |
| B A N K S Y |
I can confirm that we will be having a regional arts and health event here at MMU on October 29th 2010, where we will expand on the idea of a North West Manifesto/Big Society, and I will provide more details as they emerge. This may well include some input from the new economics foundation on the Five Ways to Well-Being.
And a big reminder, if you want to comment on the North West Health and Well-Being Alliance, please email me comments by August 6th so I can present a cohesive voice for the sector. And if a Year of Wellbeing is being proposed for the North West Region, the arts should be at the heart of this emerging public health agenda.
As I promised at the evening session, here are some links to things we discussed and some anonymous comments that we might expand on.
Arts and Business and the National Campaign for the Arts have jointly formed a Culture Forum to lobby government and explore these Big Society themes further. 3 of the 26 forum members include representatives of the arts/health sector, including the Chair.
The lecture that I described about Politics of the Common Good by Professor Michael Sandel as part of the Reith Lectures 2009, should be here: www.bbc.co.uk/programmes/b00lb6bt
The wonderful Public Health pioneer Mark Burns, who harnesses many elements of popular culture has a website here:
Programme for Government, May 2010:
Polly Toynbee commenting on Art and the Big Society:
new economics foundation and Five Ways to Well-Being:
The Great Transition link:
http://www.neweconomics.org/publications/great-transition
demos link to Civic Streets report:
Mark Thomas presents The People’s Manifesto:
Museum of Modern Art, dementia programme:
A link to the inspirational Dennis Potter, which is too short, but you can dig deeper on youtube, because he’s worth it…
Orange RockCorp, where Orange are already awarding community activists:
I described the drive to develop a National Arts and Health Forum, well here’s the link:
Some comments that you may want to further expand on…
‘What stops us from making plans to demonstrate or collaborate?’
‘The mental health impact of increased worklessness will be huge. How will the government address these issues?’
‘People already survive without resources in impoverished areas…there has always been a big society working away.’
‘I wonder where members of the cabinet including David Cameron, volunteer?’
‘The arts will survive and thrive because by their very nature, artists are inventive and collective.’
‘The danger of the Big Society agenda is that it will diffuse everything, so that no one has the power.’
‘As people have to juggle work/life balance, where will they find extra time for new demands?’
‘There is an emphasis on payments by results, but the smaller organisations and community groups won’t be able to compete with larger organisation who have big financial reserves.’
‘How do we stay calm: why should we stay calm?’
‘The Big Society is all about addressing inequalities, but we all have varying degrees of ability in the face of poverty.’
Growth hormone, insulin resistance, body fat accumulation, and glycogen depletion: Making sense of a mysterious hormone replacement therapy outcome
Hormone replacement therapies are prescribed in some cases, for medical reasons. They usually carry some risks. The risks come in part from the body down-regulating its own production of hormones when hormones are taken orally or injected. This could be seen as a form of compensatory adaptation, as the body tries to protect itself from abnormally high hormone levels.
More often than not the down-regulation can be reversed by interrupting the therapy. In some cases, the down-regulation becomes permanent, leading to significant health deterioration over the long run. One can seriously regret having started the hormone replacement therapy in the first place. The same is true (if not more) for hormone supplementation for performance enhancement, where normal hormone secretion levels are increased to enhance (mostly) athletic performance.
Rosenfalck and colleagues (1999) conducted an interesting study linking growth hormone (GH) replacement therapy with insulin resistance. Their conclusions are not very controversial. What I find interesting is what their data analysis unveiled and was not included in their conclusions. Also, they explain their main findings by claiming that there was a deterioration of beta cell function. (Beta cells are located in the pancreas, and secrete insulin.) While they may be correct, their explanation is not very plausible, as you will see below.
Let us take a quick look at what past research says about GH therapy and insulin resistance. One frequent finding is a significant but temporary impairment of insulin sensitivity, which usually normalizes after a period of a few months (e.g., 6 months). Another not so frequent finding is a significant and permanent impairment of insulin sensitivity; this is not as frequent in healthy individuals.
The researchers did a good job at reviewing this literature, and concluded that in many cases GH therapy is not worth the risk. They also studied 24 GH-deficient adults (18 males and 6 females). All of them had known pituitary pathology, which caused the low GH levels. The participants were randomly assigned to two groups. One received 4 months treatment with biosynthetic GH daily (n=13); the other received a placebo (n=11).
The table below (click on it to enlarge) shows various measures before and after treatment. Note the significant reduction in abdominal fat mass in the GH group. Also note that, prior to the treatment, the GH group folks (who were GH-deficient) were overall much heavier and much fatter, particular at the abdominal area, than the folks in the placebo (or control) group.
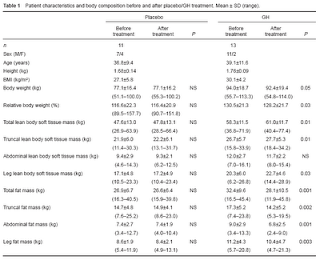
From the measures above one could say that the treatment was a success. But the researchers point out that it was not, because insulin sensitivity was significantly impaired. They show some graphs (below), and that is where things get really interesting, but not in the way intended by the researchers.

On the figure above, the graphs on the left refer to the placebo group, and on the right to the GH group. The solid lines reflect pre-treatment numbers and dotted lines post-treatment numbers. Indeed, GH therapy is making the GH-deficient folks significantly more insulin resistant.
But look carefully. The GH folks are more insulin sensitive than the controls prior to the treatment, even though they are much fatter, particularly in terms of abdominal fat. The glucose response is significantly lower for the GH-deficient folks, and that is not due to them secreting more insulin. The insulin response is also significantly lower. This is confirmed by glucose and insulin “area under the curve” measures provided by the researchers.
In fact, after treatment both groups seem to have generally the same insulin and glucose responses. This means that the GH treatment made insulin-sensitive folks a bit more like their normal counterparts in the placebo group. But obviously the change for the worse occurred only in the GH group, which is what the researchers concluded.
Now to the really interesting question, at least in my mind: What could have improved insulin sensitivity in the GH-deficient group prior to the treatment?
The GH-deficient folks had more body fat, particularly around the abdominal area. High serum GH is usually associated with low body fat, particularly around the abdominal area, because high GH folks burn it easily. So, looking at it from a different perspective, the GH-deficient folks seem to have been more effective at making body fat, and less effective at burning it.
Often we talk about insulin sensitivity as though there was only one type. But there is more than one type of insulin sensitivity. Insulin signals to the liver to take up glucose from the blood and turn it into glycogen or fat. Insulin also signals to body fat tissue to take up glucose from the blood and make fat with it. (GLUT 4 is an insulin-sensitive glucose transporter present in both fat and muscle cells.)
Therefore, it is reasonable to assume that folks with fat cells that are particularly insulin-sensitive would tend to make body fat quite easily based on glucose. While this is a type of insulin sensitivity that most people probably do not like to have, it may play an important role in reducing blood glucose levels under certain conditions. This appears to be true in the short term. Down the road, having very insulin-sensitive fat cells seems to lead to obesity, the metabolic syndrome, and diabetes.
In fact, in individuals without pituitary pathology, increased insulin sensitivity in fat cells could be a compensatory adaptation in response to a possible decrease in liver and muscle glucose uptake. Lack of exercise will shift the burden of glucose clearance to tissues other than liver and muscle, because with glycogen stores full both liver and muscle will usually take up much less blood glucose than they would otherwise.
I am speculating here, but I think that in individuals without pituitary pathology, an involuntary decrease in endogenous GH secretion may actually be at the core of this compensatory adaptation mechanism. In these individuals, low GH levels may be an outcome, not a cause of problems. This would explain two apparently contradictory findings: (a) GH levels drop dramatically in the 40s, particularly for men; and (b) several people in their 50s and 60s, including men, have much higher levels of circulating GH than people in their 40s, and even than much younger folks.
Vigorous exercise increases blood glucose uptake, inside and outside the exercise window; this is an almost universal effect among humans. Exercise depletes muscle and liver glycogen. (Fasting and low-carbohydrate dieting alone deplete liver, but not muscle, glycogen.) As glycogen stores become depleted, the activity of glycogen synthase (an enzyme involved in the conversion of glucose to glycogen) increases acutely. This activity remains elevated for several days in muscle tissue; the liver replenishes its glycogen in a matter of hours. With glycogen synthase activity elevated, glucose is quickly used to replenish glycogen stores, and not to make fat.
Depleting glycogen stores on a regular basis (e.g., once every few days) may over time reverse the adaptations that made fat cells particularly insulin-sensitive in the first place. Those adaptations become a protection that is not only no longer needed but also detrimental to health, since they lead to obesity. This could be the reason why many people initially find it difficult to lower their body fat set point, but once they lose body fat and stay lean for a while, they seem to become able to maintain their leanness without much effort.
Well, perhaps glycogen-depleting exercise is more important than many people think. It can help make you thin, but through a circuitous path.
And, incidentally, glycogen-depleting exercise causes a temporary but dramatic spike in GH secretion. This natural increase in GH secretion does not seem to be associated with any significant impairment in overall insulin sensitivity, even though glycogen-depleting exercise increases blood glucose levels a lot during the exercise window. This is a temporary and physiological, not pathological, phenomenon.
Reference:
Rosenfalck A.M., Fisker, S., Hilsted, J., Dinesen, B., Vølund, A., Jørgensen, J.O., Christiansen, J.S., & Madsbad, S. (1999). The effect of the deterioration of insulin sensitivity on beta-cell function in growth-hormone-deficient adults following 4-month growth hormone replacement therapy. Growth Hormone & IGF Research, 9(2), 96–105.
More often than not the down-regulation can be reversed by interrupting the therapy. In some cases, the down-regulation becomes permanent, leading to significant health deterioration over the long run. One can seriously regret having started the hormone replacement therapy in the first place. The same is true (if not more) for hormone supplementation for performance enhancement, where normal hormone secretion levels are increased to enhance (mostly) athletic performance.
Rosenfalck and colleagues (1999) conducted an interesting study linking growth hormone (GH) replacement therapy with insulin resistance. Their conclusions are not very controversial. What I find interesting is what their data analysis unveiled and was not included in their conclusions. Also, they explain their main findings by claiming that there was a deterioration of beta cell function. (Beta cells are located in the pancreas, and secrete insulin.) While they may be correct, their explanation is not very plausible, as you will see below.
Let us take a quick look at what past research says about GH therapy and insulin resistance. One frequent finding is a significant but temporary impairment of insulin sensitivity, which usually normalizes after a period of a few months (e.g., 6 months). Another not so frequent finding is a significant and permanent impairment of insulin sensitivity; this is not as frequent in healthy individuals.
The researchers did a good job at reviewing this literature, and concluded that in many cases GH therapy is not worth the risk. They also studied 24 GH-deficient adults (18 males and 6 females). All of them had known pituitary pathology, which caused the low GH levels. The participants were randomly assigned to two groups. One received 4 months treatment with biosynthetic GH daily (n=13); the other received a placebo (n=11).
The table below (click on it to enlarge) shows various measures before and after treatment. Note the significant reduction in abdominal fat mass in the GH group. Also note that, prior to the treatment, the GH group folks (who were GH-deficient) were overall much heavier and much fatter, particular at the abdominal area, than the folks in the placebo (or control) group.

From the measures above one could say that the treatment was a success. But the researchers point out that it was not, because insulin sensitivity was significantly impaired. They show some graphs (below), and that is where things get really interesting, but not in the way intended by the researchers.

On the figure above, the graphs on the left refer to the placebo group, and on the right to the GH group. The solid lines reflect pre-treatment numbers and dotted lines post-treatment numbers. Indeed, GH therapy is making the GH-deficient folks significantly more insulin resistant.
But look carefully. The GH folks are more insulin sensitive than the controls prior to the treatment, even though they are much fatter, particularly in terms of abdominal fat. The glucose response is significantly lower for the GH-deficient folks, and that is not due to them secreting more insulin. The insulin response is also significantly lower. This is confirmed by glucose and insulin “area under the curve” measures provided by the researchers.
In fact, after treatment both groups seem to have generally the same insulin and glucose responses. This means that the GH treatment made insulin-sensitive folks a bit more like their normal counterparts in the placebo group. But obviously the change for the worse occurred only in the GH group, which is what the researchers concluded.
Now to the really interesting question, at least in my mind: What could have improved insulin sensitivity in the GH-deficient group prior to the treatment?
The GH-deficient folks had more body fat, particularly around the abdominal area. High serum GH is usually associated with low body fat, particularly around the abdominal area, because high GH folks burn it easily. So, looking at it from a different perspective, the GH-deficient folks seem to have been more effective at making body fat, and less effective at burning it.
Often we talk about insulin sensitivity as though there was only one type. But there is more than one type of insulin sensitivity. Insulin signals to the liver to take up glucose from the blood and turn it into glycogen or fat. Insulin also signals to body fat tissue to take up glucose from the blood and make fat with it. (GLUT 4 is an insulin-sensitive glucose transporter present in both fat and muscle cells.)
Therefore, it is reasonable to assume that folks with fat cells that are particularly insulin-sensitive would tend to make body fat quite easily based on glucose. While this is a type of insulin sensitivity that most people probably do not like to have, it may play an important role in reducing blood glucose levels under certain conditions. This appears to be true in the short term. Down the road, having very insulin-sensitive fat cells seems to lead to obesity, the metabolic syndrome, and diabetes.
In fact, in individuals without pituitary pathology, increased insulin sensitivity in fat cells could be a compensatory adaptation in response to a possible decrease in liver and muscle glucose uptake. Lack of exercise will shift the burden of glucose clearance to tissues other than liver and muscle, because with glycogen stores full both liver and muscle will usually take up much less blood glucose than they would otherwise.
I am speculating here, but I think that in individuals without pituitary pathology, an involuntary decrease in endogenous GH secretion may actually be at the core of this compensatory adaptation mechanism. In these individuals, low GH levels may be an outcome, not a cause of problems. This would explain two apparently contradictory findings: (a) GH levels drop dramatically in the 40s, particularly for men; and (b) several people in their 50s and 60s, including men, have much higher levels of circulating GH than people in their 40s, and even than much younger folks.
Vigorous exercise increases blood glucose uptake, inside and outside the exercise window; this is an almost universal effect among humans. Exercise depletes muscle and liver glycogen. (Fasting and low-carbohydrate dieting alone deplete liver, but not muscle, glycogen.) As glycogen stores become depleted, the activity of glycogen synthase (an enzyme involved in the conversion of glucose to glycogen) increases acutely. This activity remains elevated for several days in muscle tissue; the liver replenishes its glycogen in a matter of hours. With glycogen synthase activity elevated, glucose is quickly used to replenish glycogen stores, and not to make fat.
Depleting glycogen stores on a regular basis (e.g., once every few days) may over time reverse the adaptations that made fat cells particularly insulin-sensitive in the first place. Those adaptations become a protection that is not only no longer needed but also detrimental to health, since they lead to obesity. This could be the reason why many people initially find it difficult to lower their body fat set point, but once they lose body fat and stay lean for a while, they seem to become able to maintain their leanness without much effort.
Well, perhaps glycogen-depleting exercise is more important than many people think. It can help make you thin, but through a circuitous path.
And, incidentally, glycogen-depleting exercise causes a temporary but dramatic spike in GH secretion. This natural increase in GH secretion does not seem to be associated with any significant impairment in overall insulin sensitivity, even though glycogen-depleting exercise increases blood glucose levels a lot during the exercise window. This is a temporary and physiological, not pathological, phenomenon.
Reference:
Rosenfalck A.M., Fisker, S., Hilsted, J., Dinesen, B., Vølund, A., Jørgensen, J.O., Christiansen, J.S., & Madsbad, S. (1999). The effect of the deterioration of insulin sensitivity on beta-cell function in growth-hormone-deficient adults following 4-month growth hormone replacement therapy. Growth Hormone & IGF Research, 9(2), 96–105.
Subscribe to:
Posts (Atom)